
EMPEREUR CHARLES V 1500/1558 Héritier des Habsbourg et de la maison de Bourgogne, Héritier de 17 couronnes
BEING BLACK, MELANIN THIS DIVINE BLESSING
www.la-melanine-une-benediction.com
SITE UNDER RENOVATION
info@la-melanine-une-benediction.com In Englishwww.melanin-a-blessing.com
ATTENTIONWE ARE ATTEMPTING TO BLOCK THIS SITE BY CALLING IT DANGEROUS. DISREGARD ANY WARNINGS, THIS SITE IS SAFE AND WELL PROTECTED with Kaspersky (the most reputable anti-virus). They do everything to prevent us from having access to our knowledge.STRONGLY RECOMMEND THIS SITE TO YOUR FRIENDS
The purpose of this site is to bring black people to self-awareness, to realize that with Africa cradle of humanity,(Africa)they are at the origin of all inventions: inventions -in all fields ofknowledge, as far back as one can trace- monopolized, copied and improved by the leucodermas who usurped them and declared themselves their inventors. Since High Antiquity, blacks have been the inventors of culture: arts, sciences, maths, philosophy, music, religion, engineering, medicine, surgery, astronomy, navigation etc... before whites stripped them of them and falsified them at their advantage. All science is related to Egypt which was a country populated by blacks.It is thanks to this black pigment present in abundance in their brain: neuromelanin,that black had and has this high capacity for creation, invention at all levels.
This site reveals the horrors and monstrosities put in place by the whites in order to degrade and reduce the blacks to the lowest level to justify their stripping, because the deficiency of the whites in this neuromelanin pigment did not allow them to equal the blacks. But neverthelessfor blacks, the purpose of this site is to be informed about them and their opponents: whites in order to be able get up and react, feel proud of themselves, grateful for their neuromelaninand their melanin, no longer allowing themselves to be reduced, degrading but having a win-win relationship in their relations with white people, no longer having this win-lose relationship which has always prevailed and continues to prevail ; the eternal winning the white, the eternal losing the black.Fueling resentment and anger towards them puts us in a losing position and has harmful effects on our health. We blacks must be diplomatic and lucidly seek our true interests in win-win relationships with leucodermas without bringing out resentment.
Isn't knowledge of one's past, of one's culture the first forms of resistance to exploitation and oppression?
Watch out, the wheel is turning, the West is in decline, the world is heading towards multipolarity. I'Africacontinent holding all the wealth of the planet, continent that does not know natural disasters,has its major role to play.Besides that our economic relations must be win-win with all our partners including Russia, China; before signing any partnership with any Western country (especially France), we must demand from them a written and signed commitment to reparations for all crimes (blood, looting, etc.) committed against us , because they have the blood of millions of Africans on their hands. We must also set up our own International Criminal Court to try all those Western criminals who abused us without mercy.We will be globally respected the day we command and inspire respect.
Dear visitors,see for yourself! : my videos are often deactivated, although very active on you tube, my visit counter had been removed (I put it back), as well as certain images. Would revealed truths bother?Recommend this site to those around you



Read the book ''Les Noirs 1ers Européens''
Sold by theTamery bookstorein Paris. General Library Guadeloupe The true history of blacks in Europe. 5th edition
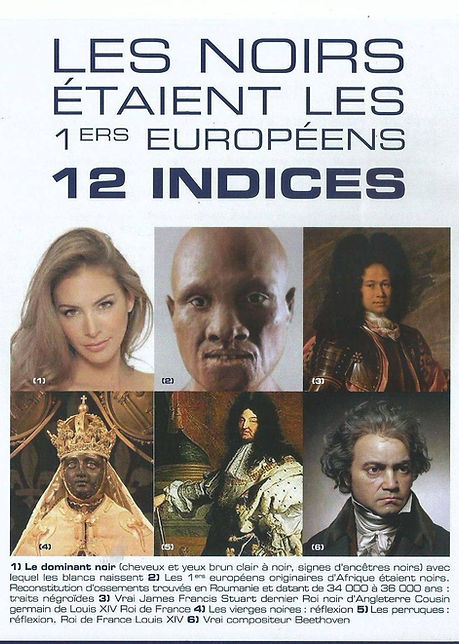
" The manipulation of the past is an instrument of power: the winner to legitimize his conquests, the oppressor to justify his violence alter, disguise the past of their victims. Source: B Saint-Sernin: Political Action according to SimobornWeil pp53
-There are two Histories: the official, lying history that is taught; then the secret history, where are the true causes of the events: a shameful history "(Honoré de Balzac, writer)
We Blacks MUST KNOW that we have been victims since the 18th century by the leucodermas (the whites) of the most vast and monstrous impersonation of our kings, queens and famous people of Europe, that history has ever known. We are also victims of the greatest and diabolical falsification of history ever carried out. The leucodermas have done this diabolical work of make-up and crime with the help of their globally present secret societies.
Isn't knowledge of one's past, of one's culture the first forms of resistance to exploitation and oppression?
The Myth of Chronic Vitamin D Deficiency in Blacks
The Myth of Chronic Vitamin D Deficiency in Blacks
Vitamin D deficiency: symptoms


eumelanin(black skin melanin)is essential for UV protectionwhich cause skin cancer by damaging DNA. Black skin blocks twice as much UV rays as white skin. Melanocytes in black skin are more resistant to damage and supply melanin more sustainably. Melanin also has an action against free radicals (chemical molecules contributing to aging and disease) Dark skin, which contains more melanin than light skin, is better protected against UV-induced damage; melanin in black skin is twice as effective compared to white skin in inhibiting UV radiation.
Thanks to melanin (eumelanin), black skin absorbs UV rays from the sun, while white skin devoid of melanin reflects UV rays from the sun and therefore cannot fix calcium because it is the vitamin D produced by the exposure to the sun which allows its fixation in the bones. The consequence of this lack of calcium fixation in whites will cause osteoporosis (bone disease).
Vitamin D is produced by exposure to the sun.The skin is believed to convert sunlight into vitamin D because of 7-dehydrocholesterol (lipid in blood plasma converted to vitamin D3 in the skin). Vitamin D (D2, D3) has many benefits for humans both physiologically and emotionally. Here are the most important: It increases the strength of bones and teeth by allowing the body to fix calcium, Strengthens the immune system, Reduces the risk of cancer, Fights against heart disease, Reduces inflammation, Reduces the risk of diabetes type 2, Blocks radiation from radiation, Keeps you mentally alert, Works against occasional depression, Encourages emotional stability.
Dark skin, which contains more eumelanin than light skin, is better protected against UV-induced damage, and eumelanin (melanin in blacks) is considered superior to pheomelanin (pseudo-melanin in whites) in its photoprotective properties.
However, skin pigmentation has been reported to significantly reduce vitamin D3 synthesis, black-skinned people require at least 6 times greater amounts of UV (sun) radiation to increase circulating levels. of vitamin D3 than those with white skin. It has also been reported that many African Americans who live in northern regions of the United States suffer from severe vitamin D deficiencies despite vitamin D supplementation; It has been reported that black people need vitamin D3 doses 6 times higher than white people (Brenner and Hearing report 2008:540-541)
Additionally, studies show that blacks have bones that are denser and less prone to fractures and osteoporosis than whites (report O'connor et al., 2003:263)which should not be the case if we are generally deficient in vitamin D.
This should impress upon us the importance of considering race and ethnicity in the study of the human body and medicine. If you simply take a race-blind approach that assumes everyone is the same, you will inevitably arrive at flawed concepts and practices. This amounts to realizing that white people's vitamin D needs are 6 times greater than black people's.
Furthermore, why rely on data exclusively concerning the white race to determine the biological needs of blacks when we know that in general blacks have fewer diseases and deficiencies than whites, are also more resistant and robust; and this thanks to the antioxidant properties of their melanin. We saw this universally during the covid 19 pandemic. African populations were much less affected than Europeans.
THE BLOOD: Racial Differences in Hemoglobin Concentration: Measurements of Iron, Copper, and Zinc(www.ajcn.org )
It is now scientifically established that blood can be racially or ethnically specific.
Most people are familiar with the eight main blood types: A, B, AB and O, which can each be positive or negative (the Rh factor). These are determined by genes, and which group you are from depends on what combination of proteins and sugars - antigens - cover your red blood cells. The International Society of Blood Transfusion lists 360 known antigens, but the combinations are infinitely more. Many do not affect routine blood transfusion, although all have been discovered due to causing a compatibility issue.
Transfusion
A successful blood transfusion is based on the same principle. If the transfused blood has an antigen that you are missing, your body may react badly. In extremely rare cases, the reaction can be fatal; and even if it doesn't, it can damage the immune system in people who are already weakened by their condition. In addition, you will make an antibody, a kind of immune soldier, which will help to recognize the same antigen better next time. Patients who need regular blood transfusions – those with sickle cell disease, thalassemia or leukemia, for example – continue to create antibodies and may face a decreasing need for appropriate blood because they continue to create antibodies .
We know that not everyone has the same blood, because there are many different types of blood and these types are important for anyone who needs a blood transfusion. Race is important in this context, because people of the same race are more likely to have the same blood type.
Racial Differences in Hemoglobin (Hb) Concentration: Measurements of Iron, Copper, and Zinc
Nutritional surveys have shown that Hb levels in blacks are consistently lower than those in whites. This difference does not appear to be related to socioeconomic dietary differences or differences in inherited disorders such as sickle cell disease. We studied 47 black subjects and 63 white subjects from hospital employees. The average Hb of black men was 0.9 g/dl lower than that of white men. The average Hb of black women was 0.5 g/dl lower than that of white women. This difference was not associated with differences in serum iron, iron binding capacity, or transferrin saturation. White women's ferritin values were significantly lower than values seen in white men, but similar differences were not observed between black men and women. The explanation for this is unclear although it may be related to sample size or differences in menstrual status. Copper levels were lower in white men than in any other group, and zinc levels were essentially similar between racial groups. The red blood cells of blacks were also smaller in quantity than those of whites. This difference could not be explained by disordered Hb synthesis. These observations confirm that Hb concentrations in black men and women are lower than in their white counterparts. This difference cannot be explained by differences in iron, copper or zinc intakes. Furthermore, Hb measurements in nutrition survey populations reflect iron status as only one of many variables and should not be used as the sole assessment of iron nutrition. It is also found that white blood cells are more numerous in whites.
In a large population of African American and white subjects undergoing health screening, we found that whites had higher hematocrit levels, higher hemoglobin levels, higher CVD, higher TS and lower serum ferritin levels than African Americans. The white blood cell count of African Americans was lower, and this difference was mainly due to a decrease in the number of granulocytes, whereas the absolute lymphocyte count was actually higher among African Americans. These data were consistent with the observations of others (see Perry et al2 for a detailed review of hemoglobin data). Although it has been proposed that the difference in hemoglobin levels may be mainly due to socioeconomic and nutritional factors, most studies suggest that there are other causes, most likely genetic, that account for the difference. . Perry et al2 provided evidence that the difference in hemoglobin is not due to iron deficiency. High levels of serum ferritin have been found in African Americans in previous studies. Although the cause of this difference between African American and white subjects is not fully understood, it is likely to have a genetic basis, as familial segregation of ferritin levels has been demonstrated in Africans.
From these observations one could deduce that in general the biological needs of whites would be higher than those of blacks.
However, we must not forget that the antioxidant melanin playing a significant role in the fight against free radicals is very present in the blood, organs, tissues of blacks, unlike whites. Couldn't these biological differences also be explained by its presence?